Top 5 Devices Ranked
by Clinical Evidence
We tested and scored 50+ devices on wavelength accuracy, delivered irradiance, and the peer-reviewed evidence behind each one. No marketing claims — just the data.
What Is Red Light Therapy for Skin?
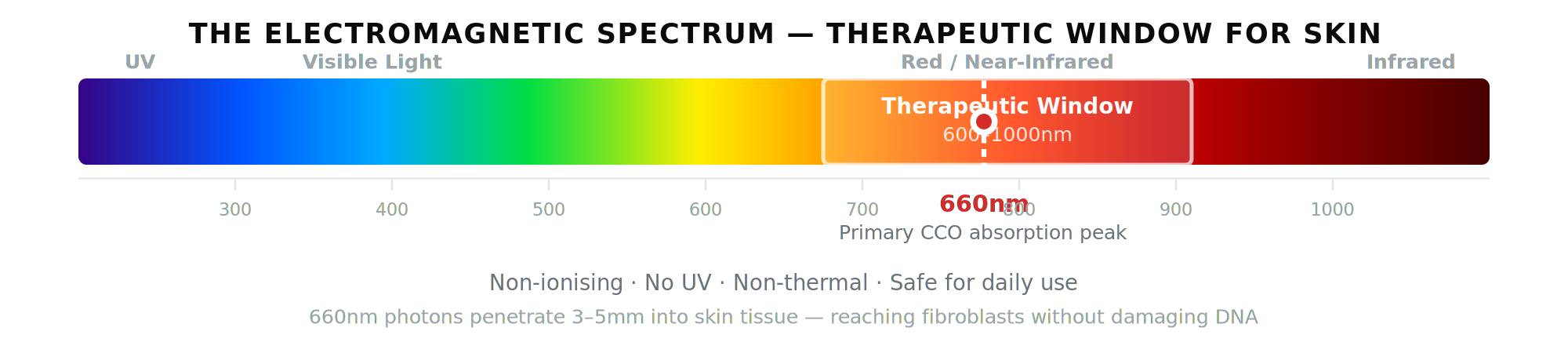
Red light therapy — clinically termed photobiomodulation (PBM) — is the therapeutic application of specific wavelengths of visible red and near-infrared light to biological tissue. Unlike UV light, which damages DNA, or heat therapy, which works through temperature change, red light therapy operates through a precise photochemical mechanism at the cellular level.
The critical wavelength for skin is 660nm. At this wavelength, photons penetrate 3–5mm into skin tissue — reaching the reticular dermis where fibroblast cells produce collagen. No topical skincare product can reach this depth. 660nm light does it non-invasively.
This is not a wellness trend. Red light therapy has been studied for over 50 years, has more than 4,800 peer-reviewed publications, and was awarded the Nobel Prize in Physiology or Medicine in 1903 in its earliest form (Niels Finsen, light therapy for lupus vulgaris).
How Does Red Light Therapy Work at the Cellular Level?
The mechanism is documented to molecular detail. Here is what actually happens when 660nm photons reach your skin.
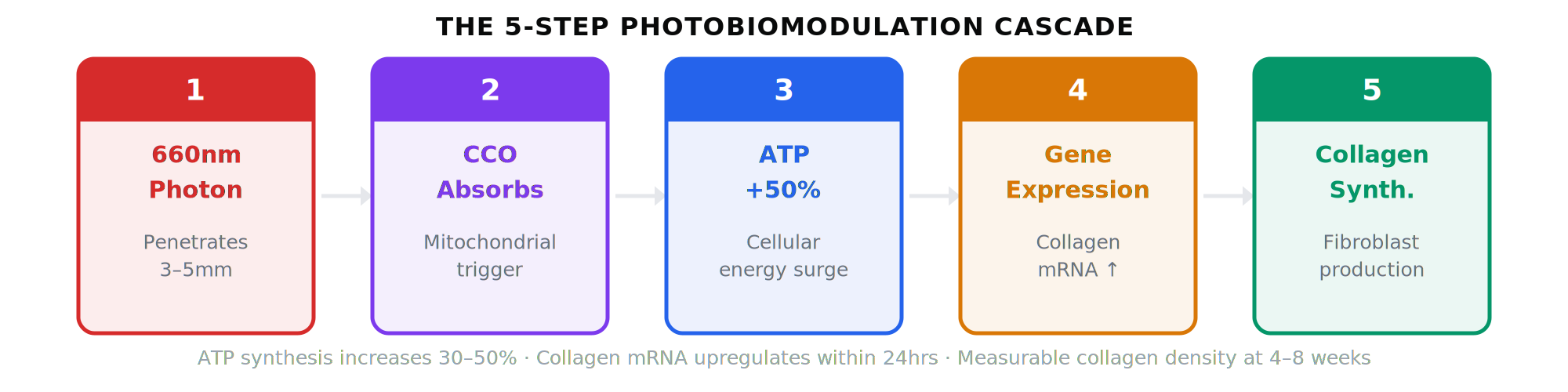
The 5-step photobiomodulation cascade
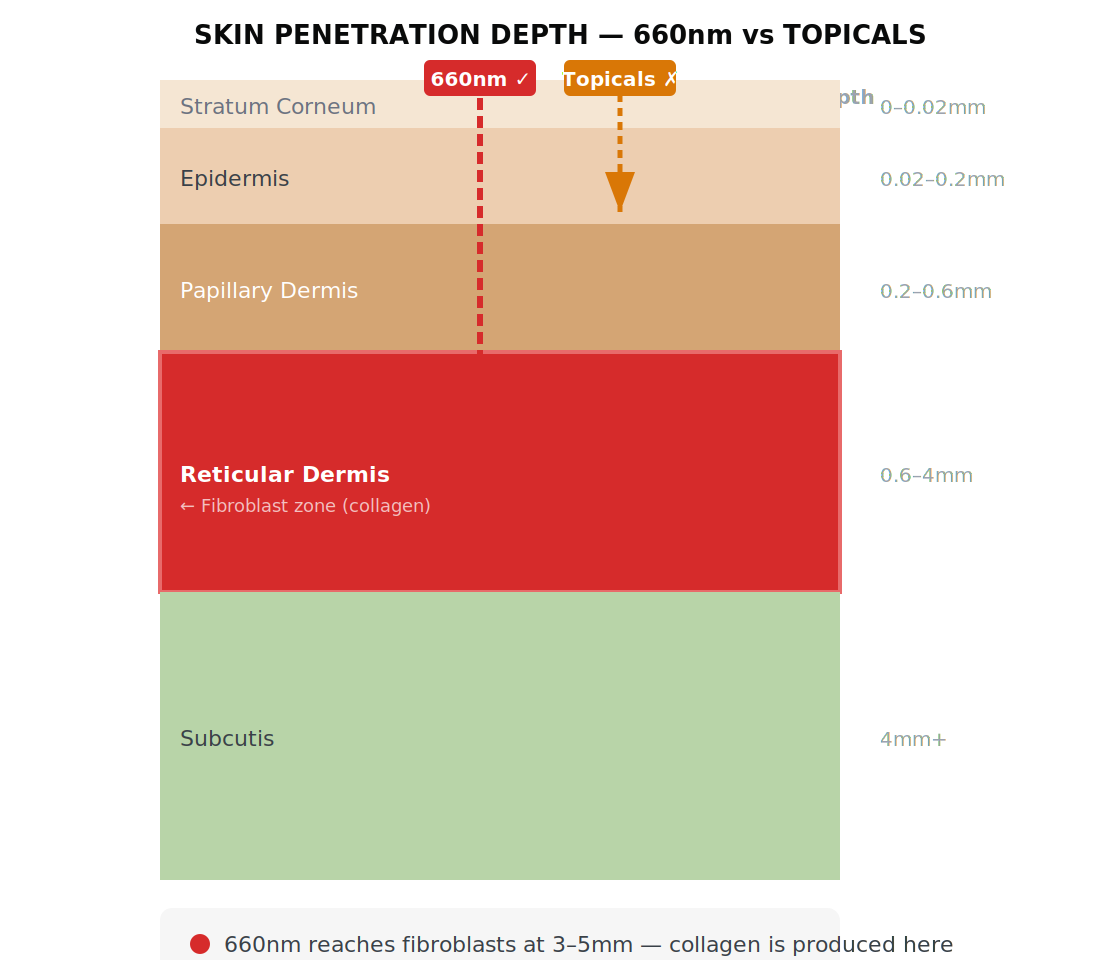
Why topicals can’t reach fibroblasts
The stratum corneum is a tightly packed barrier of dead keratinocytes. Molecules above ~500 Daltons cannot passively diffuse through it. Retinol (286 Da) and Vitamin C (176 Da) are physically stopped in the upper epidermis. Hyaluronic acid (4 million+ Da) never enters the skin at all. 660nm light passes through the entire barrier and reaches the collagen-producing cells non-invasively.
The Research: What Peer-Reviewed
Studies Actually Show
Red light therapy has 4,800+ peer-reviewed publications. Here is what the highest-quality evidence shows for skin applications specifically — double-blind RCTs with biopsy-confirmed outcomes.
Why this evidence is high quality
The studies cited here all meet three criteria that separate strong evidence from weak: (1) double-blind methodology — neither participants nor assessors knew who was in the active treatment group; (2) objective outcome measures — profilometry, punch biopsy, and validated scoring scales rather than self-report; (3) publication in peer-reviewed dermatology journals — independent editorial scrutiny.
What the evidence does not show
Red light therapy does not replace medical treatment for severe acne, chronic rosacea, or significant skin laxity. It is not effective for sun damage at depth (laser resurfacing is more appropriate for established photoageing). It will not correct structural asymmetry or replace filler or Botox for volume loss.
What it does well: Collagen synthesis stimulation, anti-inflammatory effects on redness and acne, and maintenance of dermal density with consistent long-term use.
What to Look For When Buying
a Red Light Therapy Device
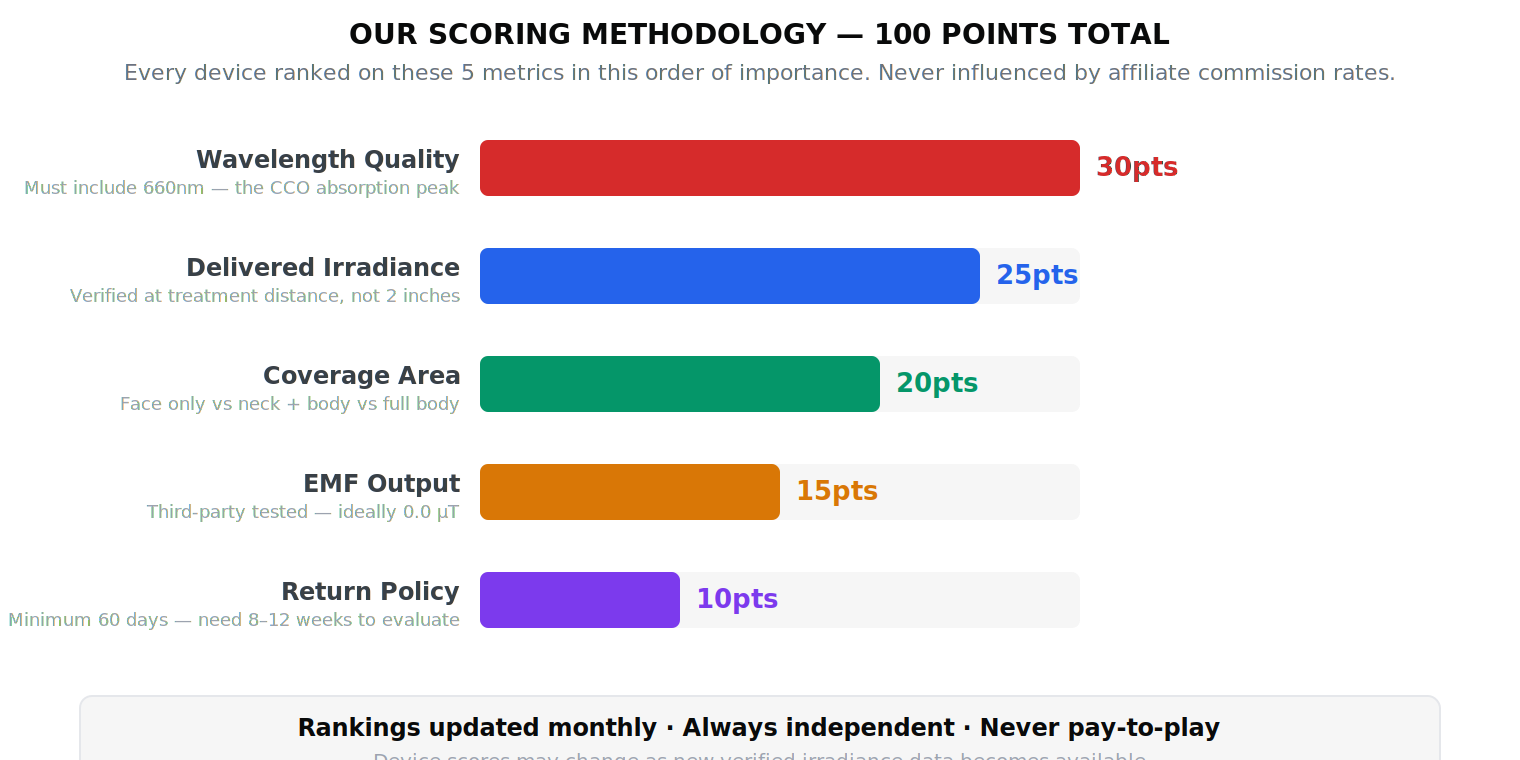
The market has hundreds of devices. Most produce no clinical outcome. These five metrics determine whether a device will actually work — in the order they matter.
#1 Wavelength — the most important factor
The device must include 660nm. CCO absorption peaks at 665nm — this is the wavelength that drives fibroblast activation and collagen synthesis. Devices that only emit at 630nm, 633nm, or 700nm are measurably less effective. Some devices add 830nm for deeper dermal support — this is beneficial but secondary.
#2 Irradiance (delivered, not claimed)
Irradiance is the power density arriving at skin surface, measured in mW/cm². The therapeutic minimum is approximately 30 mW/cm². The problem: most brands report irradiance at 2–4 inches, but you use the device at 6–12 inches. Irradiance follows the inverse square law — double the distance = quarter the power.
#3 Coverage area
Face masks treat the face only. A good panel treats your face, neck, décolletage, and upper body simultaneously. If your concerns extend beyond facial skin — or if you want to treat multiple areas in a single session — a panel is the better choice on this metric.
#4 EMF output
At high irradiance (100+ mW/cm²), some panels produce measurable electromagnetic fields. Look for third-party EMF test data — not manufacturer claims. Devices built on isolated driver boards with proper shielding can achieve essentially zero EMF output at therapeutic irradiance.
#5 Return policy
RLT results take 8–12 weeks. A 30-day return window is effectively useless — you cannot evaluate efficacy in 30 days. Minimum acceptable: 60 days. Several devices in our top 5 offer 60–90 day trials. One brand (Platinum LED, #4) charges a 20% restocking fee — the only device in our list with a return cost.
LED Face Masks vs Panels:
Which Should You Choose?
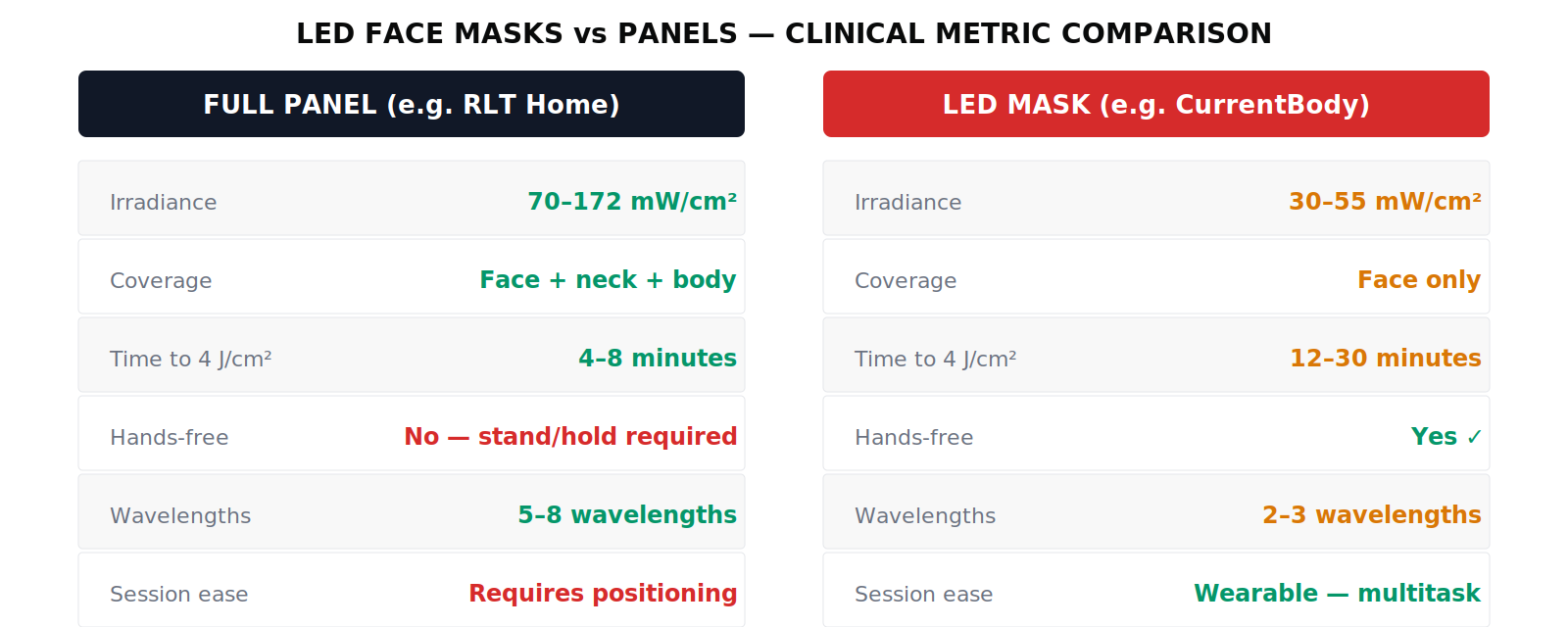
This is the most common question we receive. The honest answer is: panels outperform masks on almost every clinical metric — but masks have one genuine advantage that matters for some people.
The one real advantage of masks: compliance
The single strongest predictor of red light therapy outcomes is consistent daily use. A hands-free mask you wear for 10 minutes during your morning routine will outperform a more powerful panel you use sporadically. If a mask is the only device you will actually use every day, it may be the right device for you.
Where masks fall short clinically
Irradiance: Most masks deliver 30–55 mW/cm². At 40 mW/cm², a 10-minute session delivers only 2.4 J/cm² — below the 4 J/cm² therapeutic minimum. You would need 17 minutes at minimum to reach a clinical dose. Most mask users do not know this.
Coverage: Masks treat the face only. Neck, décolletage, and body remain untreated. If your concerns extend to the neck or beyond, a mask cannot address them.
Wavelength: Most masks use 633nm or 630nm — close to the 665nm CCO peak but not precisely on it. The physics favour 660nm. The difference is not enormous, but it exists.
Top 5 Red Light Therapy Devices
for Skin — Ranked & Reviewed
Scored on 5 clinical metrics. Rankings are never pay-to-play — only the data determines position.